Normally the food we eat moves from the esophagus into our stomach where digestion continues. In time, the bolus of food moves into the first part of the small intestine, the duodenum, where the acid pH of the stomach is neutralized and chemicals from the duodenum, liver, gall bladder, and pancreas assist with digestion and absorption of nutrients. The food then moves to the second part of the small intestine, the jejunum, where digestion and absorption continues.
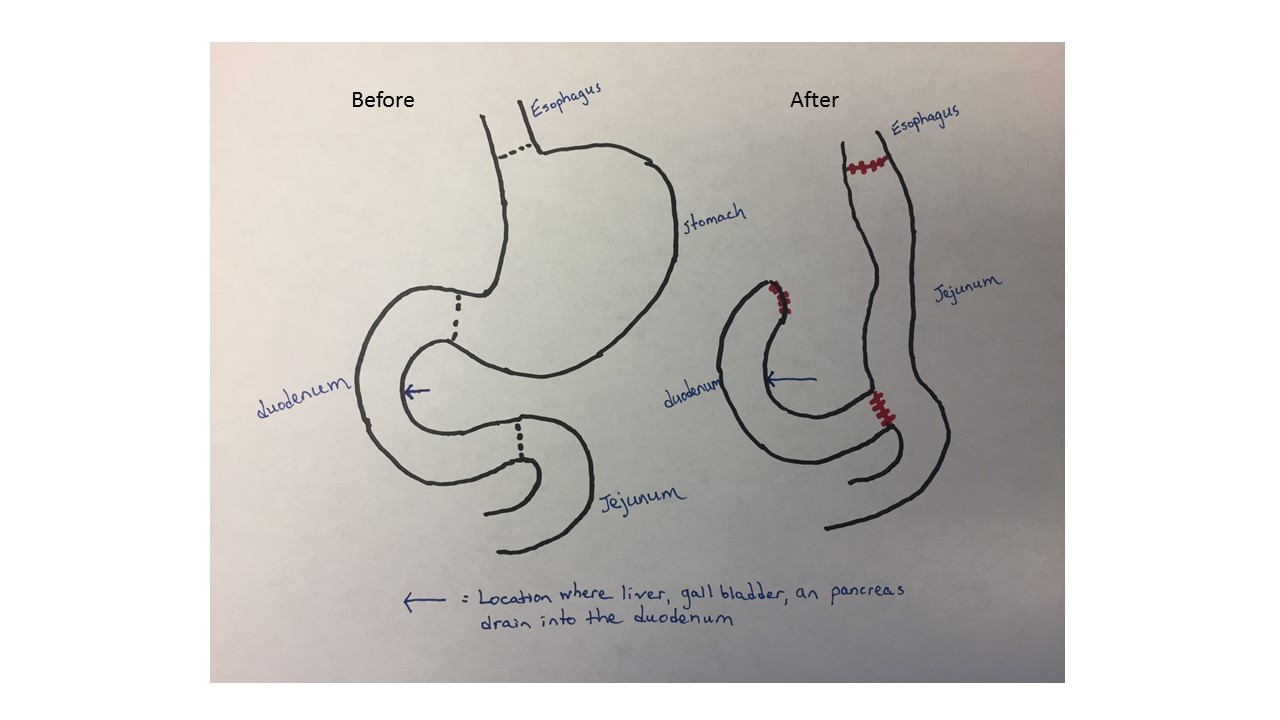
The procedure I will have is similar to the roux en y procedure that people undergo to lose weight through bariatric surgery with the addition of removing the stomach completely. The stomach will be disconnected from the esophagus and duodenum and removed. This is not a laproscopic procedure. The end of the duodenum will be sutured shut. The small intestine will be cut near the junction of the duodenum and jejunum and the proximal end of the jejunum will be attached to my esophagus. The distal end of the duodenum will then be attached to part of the jejunum.
So you can see that I will be losing a big sack and what I eat will enter a much smaller tube. I will have to substitute my 3 regular meals with 5 or 6 small meals throughout the day. I will start with liquids and soft foods then slowly add to my diet. Eventually, I will be able to eat whatever my body can tolerate. Sugars can be a problem. Some patients become lactose intolerant. It will be trial and error. I need to make sure I get enough protein to maintain muscle mass. One of the important functions of the stomach is its production of intrinsic factor. This allows the body to absorb vitamin B12. Vitamin B12 is important for the production of normal red blood cells. A B12 or iron deficiency can lead to anemia. If this happens, I will have to take oral B12 and iron supplements. If that doesn’t work I would get monthly injections. It could take up to a year for my body to adjust to the new regiment.
